
Skiing isn’t for the faint of heart.
Neither is subjecting oneself to what is coyly referred to as “America’s Health Care System.” Hold that thought while I elaborate on point one, that a lifetime devoted to skiing is hard to navigate without occasionally experiencing a consequential impact with the planet or some other immovable object attached to it. If you ski long enough, you will eventually learn the meaning of terms like “laminectomy” and “stenosis.” If you don’t know these terms yet, please bear with me while I bring you quickly up to speed with those who know them all too well.
As far as I know, there wasn’t any one big crash that led me to my first laminectomy. It was the accumulated stress of thousands of reckless bump runs that eventually caused L4/L5 to collapse, releasing its gooey contents into the surrounding spinal column. Just to remind you that all is not well in your lower back, the rogue material sends out signals that make walking difficult and golf excruciating. It takes a few months of this torture to qualify for an MRI which makes the problem impossible to miss.
Even though my back surgeon was reputably the best in Reno, he botched the first operation, inexplicably leaving a large mass of roving goo to wrap itself around my spine, mandating (after a couple of months of eye-watering agony) a second procedure that removed the remaining loose lubricant and rendered me uninsurable when I lost my job and its attendant medical coverage. Gotta love a “system” that kicks anyone to the curb for having the audacity to use it.
My second major spinal injury wasn’t induced by sustained abuse of my lumbar region, but by a single bad decision that nearly broke my neck. It was early in a low-snow year, first run of the day off KT-22. I was checking the tune on Head skis I’d brought to an industry event, planning to run laps until I’d checked out the lot of them. I didn’t make it past ski one, which happened to be a Non-FIS GS race model, so I wasn’t poking my way downhill. As I approached the base area, I took a wide turn, going slightly outside the narrow ribbon of groomage, my eyes fixed on the KT lift where I planned to switch skis.
I never made it that far, for unbeknownst to me the trail was only lightly dusted with snow, so when I went right, I steered into a long pit of barely covered rocks. Both skis were ripped violently off my boots and I was fired forward in a low-trajectory arc. Some instinct reminded me to get my chin up before I used my face as a brake pad. (The skis, BTW, did not survive this event.) As I spun slowly to a stop, it seemed my only serious injury was to my dignity, but I would later discover I had damaged C2/C3 rather nastily. Eventually, I got an epidural injection that magically reduced the swelling in my neck in the time it took me to swing my legs over the side of the operating table. (Best medical intervention ever.) But of course, C2/C3 would never be quite the same.
Flash forward a couple of decades to this past season, and my old spinal injuries began to re-surface. The first manifestation was stiffness in my neck, such that I could only turn my head to the right. Big deal, I could cope with that. What I failed to realize was the pain in my neck was disguising a bigger problem in my old lumbar injury. When most of what made L4/L5 a functioning shock absorber was removed, it left L3/L4 to do the work of two, wearing it down to the nubs. Sometime during my last of round of golf, it quit.
It did not go quietly. To make sure I didn’t ignore it any longer, it shifted relative to its neighbor, grinding any remaining nerves in what was already a narrow canal into an angry, noisy pulp. To help you visualize the narrowing of the spinal pathway my nerves were dealing with, imagine The Three Stooges all trying to get through a doorway at the same time. That’s stenosis.
My pain specialist suggested ablation, a barbaric technique that kills the pain messenger rather than addressing the root problem. To prepare the patient for what will be a brutal series of nerve-killing injections, a local anesthesia is injected first, an exercise in applied agony apparently meant to tenderize the patient before sending in the nerve-killing crew.
I’m making it sound better than it actually was. But the ablation turned out to have two benefits: first and perhaps foremost, it allowed me to lay still in an MRI tube the following day, which I probably wouldn’t have managed without it. The second benefit took a while to take effect, but as I sit here at my keyboard, I’m grateful for the relative calm in the storm that continues to rage in my lumbar region.
You see, for the month between the onset of the vertebral displacement and the ablation, the remains of my lumbar region sent out distress signals at every opportunity. The electrical storm in my back would fire off salvo after salvo of biomechanically sourced lightning at a pain level that was not easily disguised. Not only did I shuffle about like an arthritic Quasimodo, the party in my back would occasionally fire off a suite of violent shocks, accompanied by verbalizations that went something like, “Ow, fuck, oh shit, JESUS H. CHRIST! oh, oh, oh, oh, FUCK ME NAKED! OW, OW, OW!” On the third “OW!,” my knees would buckle and I’d have to grab whatever was nearest to keep from hitting the floor. (My cat, Oscar Wilde, kept his distance during these outbreaks. Smart kitty.)
Once medial professionals began mucking around in my back, they found all sorts of possible ailments to help keep me awake at night. I had a CT scan of my chest and abdomen, along with a bone marrow biopsy (super fun!), because some savant thought he saw perhaps some incipient cancer growing in my back. (This diagnosis has since been relegated to a back burner due to a lack of supporting evidence.) I’ve had enough blood drawn to sate an extended family of vampires, and every inch of me scanned by one device or another. After a day and half in the hospital and more tests than I took at Yale, the verdict was, I’m fine.
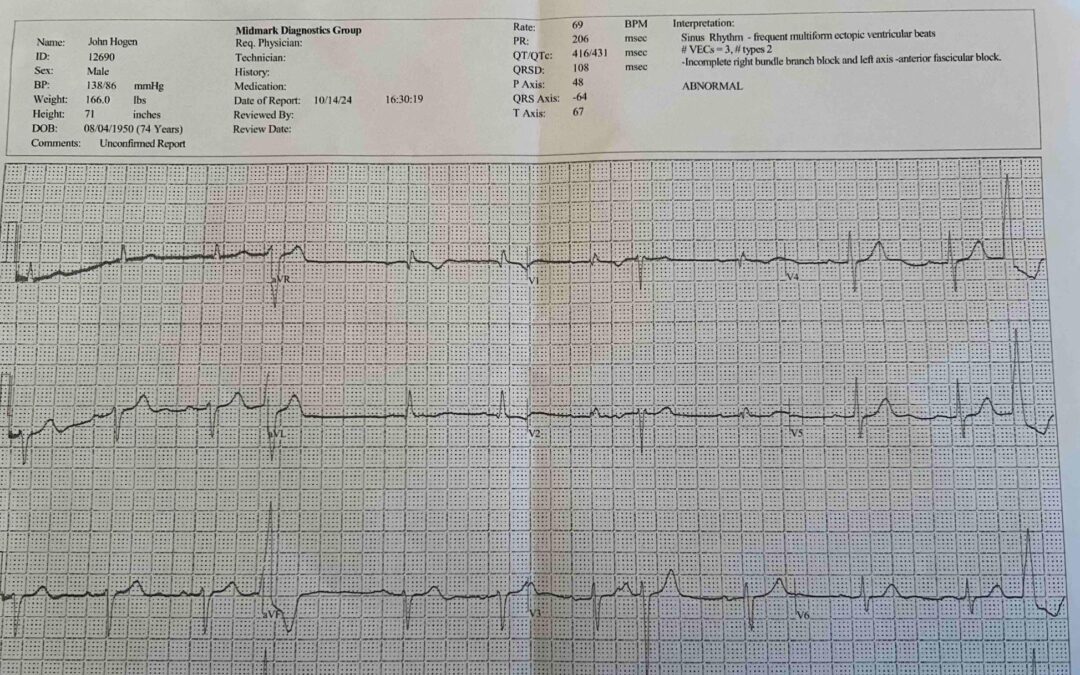
I still had to see a heart specialist because of a slight abnormality in my EKG which concerned my primary care physician, who wouldn’t give me clearance for my back operation without yet another specialist’s okay. I finally got said clearance last Friday, which now goes back up the chain to my primary and thence to the back surgeon. I hope to finally get on his docket next week and on his operating table some time shortly thereafter.
The perspicacious Dear Reader may well wonder how I ended up diverted to the hospital when my objective was simply to schedule a minimally invasive (their words, not mine) back surgery. That was my doing. I was wandering my yard when I began to feel woozy, as if a fog had settled on my brain. I couldn’t figure out why I was feeling so oddly disconnected and whatever my condition was, it was worsening. I didn’t want to pass out on the lawn, leaving my 100-pound wife to cope with my unresponsive body. So, I called 911 and was duly delivered into the medical-care machinery.
As noted above, I was checked for everything imaginable and emerged with a clean bill of health. Yet as I was being wheeled to the curb, I couldn’t suppress the sensation that something still wasn’t quite right. It wasn’t until later in the day that I finally connected all the dots. The reason I checked out as A-Okay and yet still felt weirdly dizzy was that my problem was one of the few conditions I wasn’t tested for: I was constipated, which sent my vasovagal system into distress mode, causing syncope, a fancy term for feeling faint. This was the condition that knocked me unconscious while I was driving home from a ski day in the spring of 2012; I was keeping my butt clenched to prevent any sort of loose discharge occurring in my wife’s car, to the point where I blacked out. While I didn’t black out on this occasion, it explains why I didn’t feel right.
The moral of this story is that if you pass every test and still feel like crap on toast, maybe you aren’t being tested for what ails you.
The point of this story is that surgery and a little recovery time will prevent me from maintaining my usually prodigious publication schedule of Revelations and podcasts. I will still be able to answer subscriber queries about equipment and hope to attend the upcoming Masterfit University sessions in Reno, with a by-appointment-only bootfitting session slipped into the mix for good measure. Stu Winchester, of Storm Skiing Journal fame, has also invited me to a guest appearance on one of his upcoming podcasts, so my Dear Listeners have that to look forward to.
Please accept my apologies for this overly long excuse for my impending absence from your in-boxes. I shall be back as soon as I get medical clearance.
Related Articles

Is 3D Imaging a Fad or the Future?
Any serious attempt at bootfitting begins with an assessment of the customer’s feet and lower legs. This appraisal can be as superficial as measuring each foot for length or as detailed as a complete skier profile accompanied by a few basic biomechanical evaluations.
Better bootfitters gather further information from a litany of details that lie outside the scope of the usual foot-measuring device, such as a Brannock. The veteran bootfitter watches how the customer walks, sits and assumes a skiing position, for starters. The savvy fitter can even spot limb-length differences and redistribute pressure around the foot in places no measuring stick can quantify.
If this sounds like a pretty sophisticated skill set, well, it is. Yet many, if not most, prospective boot buyers approach the bootfitting exercise with the same enthusiasm they usually reserve for a root canal. Suspicions are often confirmed when the first boot proffered seems crazily short. Even the most knowledgeable fitter is obliged to re-establish his/her credibility just to move the bootfit process pass square one.

Of Podcasts, Archives & Revelations
According to my tight-knit circle of advisors, idolaters, sycophants and astrologers, I was made for this medium.
Of course, any garden-variety sycophant will whisper words of inspirational twaddle, but the faint note of sincerity I detect in the smarm-storm of platitudes meant to buck me up has proven sufficient to spur me to action. I quickly acquired a very professional looking microphone and a pop filter to knock down my fierce sibilants. To preserve my objectivity, I opted not to take any lessons, follow any tutorials or otherwise prepare myself for this venture. By the powers vested in me as the Pontiff of Powder, I declare myself to be, now and forever after, a podcaster.
I’ll give you a moment to recover.

The Making of a Skier, Chapter XI: Desperate Measures
When Head humanely, if rather brusquely, terminated my tenure in 2001, the ski business in the U.S. was already facing stiff headwinds, a brewing storm that would turn into a full-on debacle when 9/11 disrupted all commerce. I became unemployed just in time for the job market to implode.
I don’t handle inactivity well. I started writing a very long, very dreadful novel, composed a handful of scripts for Warren Miller – and later, Jeremy Bloom – to recite and scribbled batches of brochure copy and white papers for industries as diverse as accounting software, instrumented football helmets that registered concussions and risk assessment based on location.
The pickings were slim, but they wouldn’t have amounted to anything at all were it not for a little help from my friends. Andy Bigford, who I’d worked with at Snow Country, hired me for the Warren Miller gig. A college chum kindly engaged me to write white papers on accounting fraud. But it was Dave Bertoni, an erstwhile colleague from Salomon days, who joined me in creating Desperate Measures: A Training Method for Selling Technical Products at Retail.
